Introduction
According to the 2015 Global Tuberculosis Report, Indonesia has the second highest rate of tuberculosis (TB) after India. Some cases of TB develop resistance to anti-tuberculosis drugs, which is called multidrug-resistant TB (MDR-TB), and other cases are caused by non-tuberculous mycobacteria (NTM) [1]. Tuberculosis can affect both humans and animals. Mycobacterium tuberculous infects humans through droplets that are inhaled by humans. Animals can be zoonoses, which are intermediaries for tuberculous infection in humans, namely by M. bovis. The increase in TB in cattle shows the importance of conducting strict health control of livestock both actively and passively; this is TB which is a high cause of death [2].
The diagnosis of MDR-TB or NTM is time-consuming, expensive, and requires specialist examination facilities. Sputum culture takes 3-4 weeks; the sensitivity test for anti-TB drugs is also relatively complicated and takes a long time to provide information for effective treatment, and the drug of choice for MDR-TB is limited and expensive. This is also the case with NTM, which has an increasing incidence; however, diagnostic tests for NTM are rarely performed, due to its silent symptoms and the fact that specific displayed symptoms are difficult to distinguish from TB or MDR-TB. Also, NTM cases are usually accidentally diagnosed while the patients are undergoing TB examination or when TB treatment fails [3].
Chest X-ray is still routinely performed in patients with TB or suspected MDR-TB. This examination is considered inexpensive and convenient, is available in almost every hospital or healthcare facility, and allows identification of lesion characteristics. In general, chest X-ray features of TB, MDR-TB, and NTM vary widely and each has its specific characteristics. Some overseas studies have shown that in MDR-TB cases, chest X-ray displays characteristic lesions such as cavities, consolidation, nodular-infiltrates, pleural effusions, pleural thickening, hilar lymphadenopathy, and even destroyed lung/loss of volume [4,5]. Some characteristic NTM lesions on chest X-ray are cavities (thin-walled compared with TB infection) in the superior lobes of the lung, large nodular bronchiectasis (size greater than 0.5 cm), and consolidation [6,7].
The present study examined the correlation between chest X-ray lesion characteristics of MDR-TB, based on GeneXpert MTB/RIF, and NTM, based on the immunochromatographic assay MPT64 and niacin tests. GeneXpert MTB/RIF is a molecular examination technique introduced by the World Health Organisation (WHO) in 2010 for the detection of rifampicin-resistant M. tuberculosis, based on a nucleic acid amplification test (NAAT). Several studies have shown that GeneXpert MTB/RIF has a higher sensitivity (83.7%) and specificity (100%) than sputum smear microscopy or chest X-ray. GeneXpert MTB/RIF requires a much smaller sputum specimen than the sputum smear test (131 CFU/ml for M. tuberculosis), and the time required for this test is only 90 minutes, which is relatively short compared with sputum culture examination (six weeks) [8,9].
MPT64 is one of 33 proteins secreted by M. tuberculosis and is encoded by the RD1, RD2, and RD3 genes, the presence of which is used for the differentiation between the M. tuberculosis complex and NTM bacilli. Niacin/nicotinic acid is produced by Mycobacteria spp. As an essential oxidation-reduction reaction during metabolic synthesis. Niacin reagent strips are used as a qualitative identification of niacin-producing mycobacteria; M. tuberculosis is a bacterium that produces a significant amount of niacin, but NTM tests negative [10,11].
Studies comparing chest X-ray lesion characteristics of MDR-TB and NTM remain very limited in Indonesia, and most of the related overseas studies are descriptive. The present study evaluated the correlation between specific chest X-ray lesion characteristics and MDR-TB or NTM infection, based on GeneXpert MTB/RIF for the diagnosis of MDR-TB and the MPT64 and niacin tests for the diagnosis of NTM. The results of the present study can be used as an early screening test for the diagnosis of MDR-TB and NTM, which will shorten the time and cost of MDR-TB diagnosis. Characteristics of MDR-TB and NTM lesions on chest X-ray will be useful for primary screening of patients with suspected MDR-TB before subsequent, more expensive secondary screening using GeneXpert and MPT64/niacin tests for NTM. Expectations include the suppression of MDR-TB and NTM morbidity and mortality, in addition to more effective treatment.
Material and methods
Experimental subject
The present study used a cross-sectional retrospective design to obtain the correlation between chest X-ray lesion characteristics and MDR-TB and NTM infection. Experimental subjects were individuals aged 15 years or older, who had lived in the cluster area for at least one month, had clinically positive TB, had a cough for more than 14 days or were coughing up blood, or had a chest X-ray in provinces throughout Indonesia. The subjects met the inclusion and exclusion criteria. Inclusion criteria were: 1) chest X-ray diagnosis of MDR-TB; 2) chest X-ray diagnosis of NTM; 3) the final results of an MDR-TB sample, or 4) the final results of an NTM sample. Exclusion criteria were: 1) chest X-ray results with abnormalities in the pulmonary parenchyma, for instance, bronchitis, emphysematous, or a lung mass; 2) chest X-ray with massive pleural effusion; or 3) chest X-ray with extensive pneumothorax, from which pulmonary parenchyma could not be assessed.
Procedures
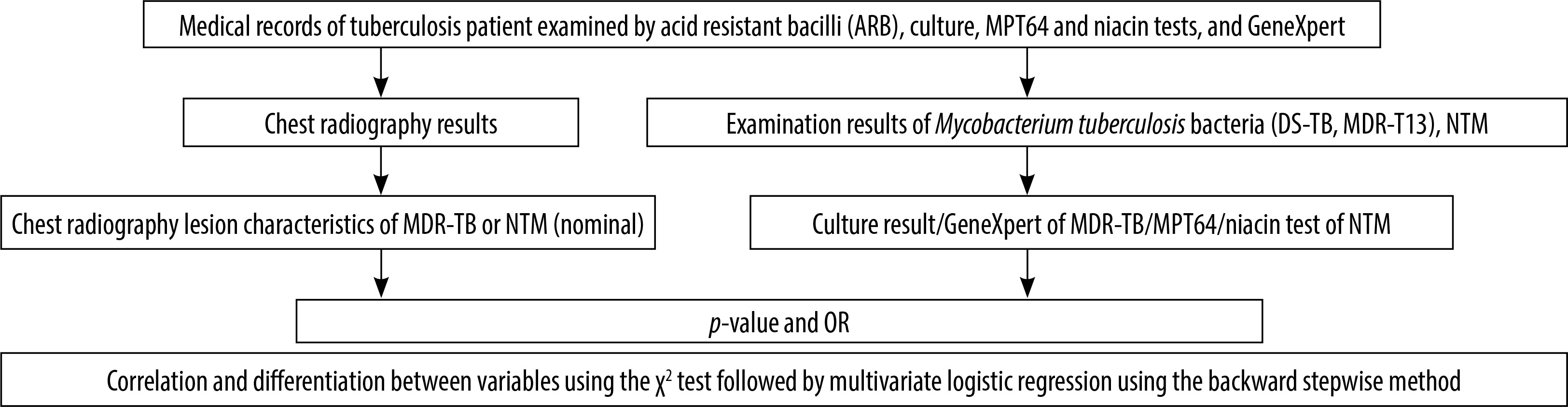
Figure 1 showed the scheme of the present study. This study used research subjects based on 15-year-old individuals who were selected based on medical records. Subsequently, chest X-ray images from M. tuberculosis bacteria (MTB) patients including drug-susceptible tuberculosis bacteria (DS-TB) and MDR-TB, also from NTM patients, were obtained. The images were investigated for lesion characteristics as well as clinical tests of culture or GeneXpert tests for MDR-TB and MPT64 or niacin tests for NTM. All data were acquired and analysed using the χ2 test followed by multivariate logistic regression using the backward stepwise method for determination of correlation and differentiation between variables.
Data acquisition
Data were obtained both primarily and secondarily. Primary data were obtained from research measured variables, both independent and dependent. The independent variables were lesion type, lesion location, and lesion extent. Lesion types on chest X-ray were: infiltrated, cavities, nodules, masses, consolidation, pleural effusion, pleural thickening, fibrosis, and calcification. Lesion locations were right upper lung, right medial lung, right lower lung, left upper lung, left medial lung, left lower lung. The lesion extent was: minimal lesions, intermediate lesions, and extensive lesions (advanced). The dependent variables were MDR-TB diagnosis including acid resistant bacilli (ARB), culture, and GeneXpert, as well as NTM diagnosis when the results showed MDR-TB and culture and subsequently MPT64 followed by niacin.
Secondary data were chest X-ray diagnosis of MDR-TB and NTM obtained from the Indonesian Tuberculosis Research Survey 2013-2014 by the National Institutes of Health Research and Development – NIHRD (ethical clearance number: KE.01.10/EC/651/2012).
Parameters
The parameters used to calculate the sample size with a certain degree of accuracy were:
Estimated TB prevalence (p): 156 per 100,000 people;
The proportion of the population that is 15 years old and over (a): 71.1%;
A 95% confidence level or α of 5%;
Relative precision (d): 20% based on WHO recommendations;
Minimum participation rate (r): 85% based on WHO recommendations;
The magnitude of the cluster (M): 500 considering the weekly operating cycle and WHO recommendations (400-800);
Design effect (deff): 1.5 (k > 0.6, approximate high cluster variation based on 2004 experience).
Based on parameters above, number of samples (were calculated using Equation 1.

Because the survey covers only adults as the eligible population, the sample size was calculated using Equation 2:

Considering the expected participation rate of 85%, the number of samples adjusted for the participation rate was calculated using Equation 3.

The number of clusters (C) needed was calculated using Equation 4.

The estimated number of participants aged 15 years and over by the 2010 census is 82,155 in 156 clauses; thus, an estimated 527 participants per cluster.
Statistical analysis
Stats Direct version 2.7.8 (Stats Direct Ltd., Cheshire, UK) and SPSS Version 22.0 for Windows (SPSS, Chicago, IL) software were used to perform statistical analysis. Normality of the data was assessed using bivariate analysis to obtain a significant correlation between chest X-ray lesion characteristics, which is a nominal/categorical scale as an independent variable, and the results of GeneXpert/sputum culture/MPT64 and niacin tests for the incidence of MDR-TB and NTM incidence, which is a nominal/categorical scale as a dependent variable (outcome). Chest X-ray correlation (lesion type, lesion location, and lesion extent) was compared with MDR-TB and NTM laboratory results using the p-value and bivariate χ2 statistical analysis followed by multivariate logistic regression using the backward stepwise method to determine lesion characteristics [7,8]. Research data, such as patient identity, was kept confidential. Data collection from the research patients was performed after obtaining a permit from the Head of the National Institutes of Health Research and Development – NIHRD. The following is the research scheme of the present study.
Results
Research subjects’ details
Research subjects’ details obtained from the national TB survey during 2013-2014 were shown in Table 1. Among the 15,127 participants who met the research inclusion and exclusion criteria, 11 individuals were diagnosed with MDR-TB and 380 with NTM.
Table 1
Distribution of national tuberculosis research subjects in 2014
| Laboratory diagnosis | Amount | Percentage | Research subjects | Percentage |
|---|---|---|---|---|
| Negative results | 13.836 | 91.47 | ||
| MTB | 426 | 2.82 | ||
| MDR-TB | 11 | 2.04 | ||
| DS-TB | 147 | 27.32 | ||
| Other | 268 | |||
| NTM | 405 | 2.68 | 380 | 70.63 |
| Other | 460 | 3.06 | ||
| Screened (+) | 15.127 | 100.00 | 538 |
Table 2 describes in detail the basic characteristics of the research subjects concerning age, gender, province of origin, urban/rural area, and educational level. The age bracket of the study subjects with the highest rate of NTM diagnosis was > 65 years old (25.68%), while that of those with the highest rate of MDR-TB diagnosis was 25-34 years old (54.55%). The majority of NTM cases were in individuals from urban areas (58.05%) as compared with those from rural areas (41.95%). MDR-TB is more common in rural areas (63.64%) than in urban areas (36.36%). Concerning the educational level of subjects with NTM, 78.52% had a relatively low educational level (uneducated/primary school/junior high school). Subjects with MDR-TB were too few (11) to be used as valid information; nevertheless, their educational level appeared to be slightly higher (junior high school and senior high school).
Table 2
Basic characteristics of the research subjects concerning age, gender, province of origin, urban/rural area, and educational level
Clinical symptoms of non-tuberculosis mycobacterium
Table 3 shows some of the clinical symptoms present at the highest percentage in NTM. All patients partly showed clinical symptoms with varying percentage values. Cough and phlegm cough were the most common clinical symptoms suffered by patients but not for other symptoms. However, the clinical symptoms of most cases of laboratory-based positive NTM are a cough (76.30%), and productive cough for a duration > 14 days (50%).
Table 3
Clinical symptoms of non-tuberculous mycobacteria patients
Non-tuberculous mycobacterial and multidrug-resistant tuberculosis lesions based on chest X-ray images
Chest X-ray images were showing the variation in NTM and MDR-TB lesions. Figure 2A and 2B show that NTM diagnosis was a consolidated feature, thin-walled cavities of less than 2.5 cm in diameter, and fibrosis in the right lung lobe. Figure 3A for MDR-TB diagnosis shows consolidation of nodules, cavities, and pleural thickening, but Figure 3B shows infiltrates and nodules. Figure 4A shows in NTM the presence of consolidated lesions located in the middle field of the right and left lung. Figure 4B shows thin-walled cavity lesions in the right medial lobe and infiltrate lesions in the left ventricular/lingula. Figure 5 shows multiple nodular lesions in the lingula or left ventricular.
Figure 2
Chest X-ray images of non-tuberculous mycobacteria lesion (indicated by black arrow). Barcode number: (A) 143137, (B) 124475
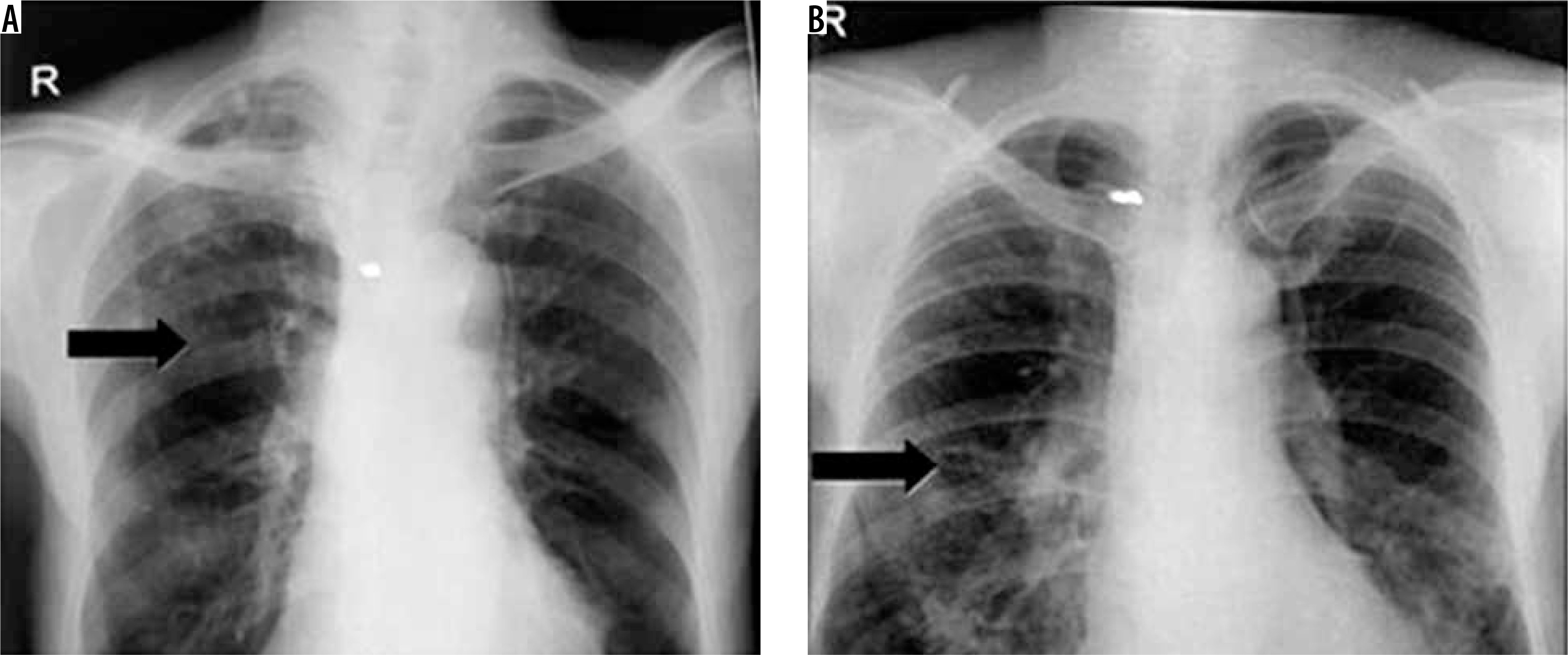
Figure 3
Chest X-ray images of multidrug-resistant tuberculosis lesion (indicated by black arrow). Barcode number: (A) 203004, (B) 223046
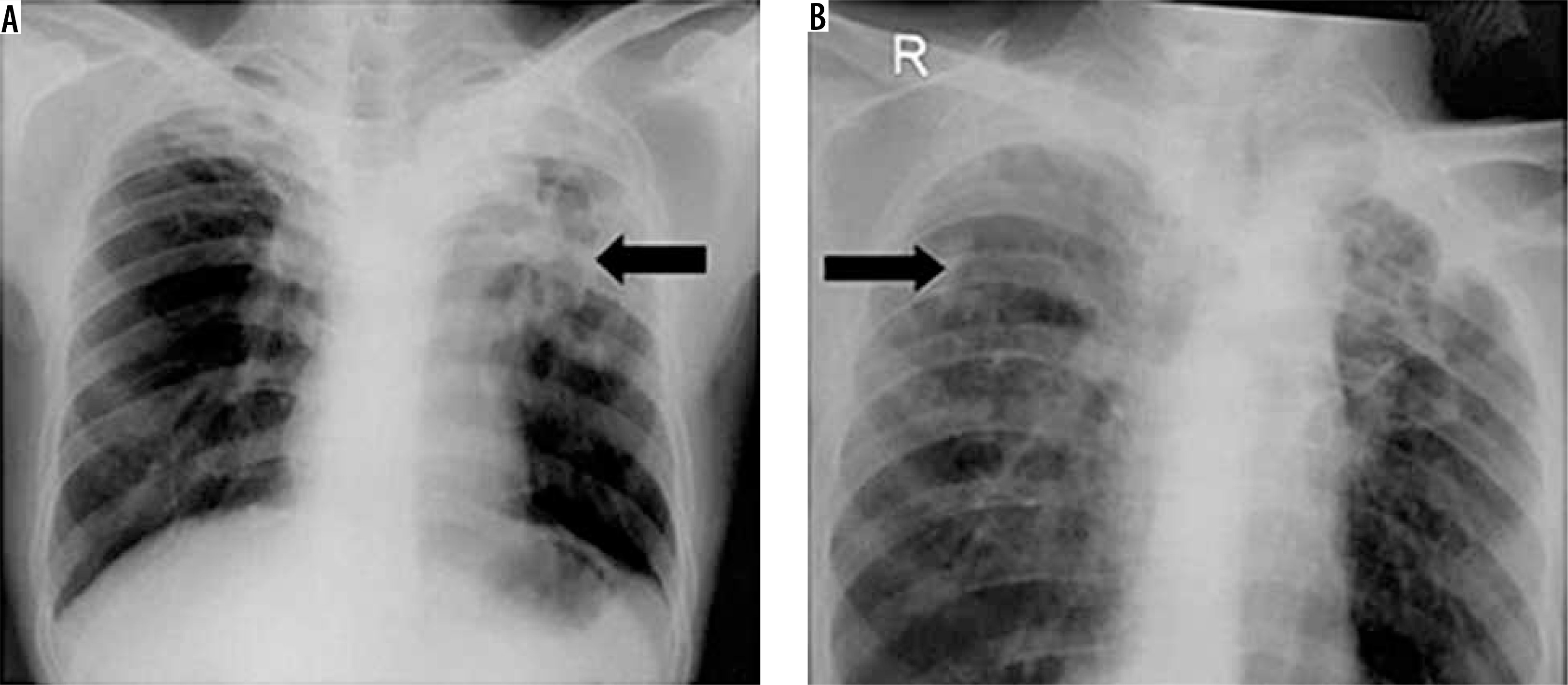
Figure 4
Chest X-ray of non-tuberculous mycobacteria diagnosis: consolidation and fibrosis in medium lobe of the lung (white arrow). A) Barcode number: 124475 and B) 120143
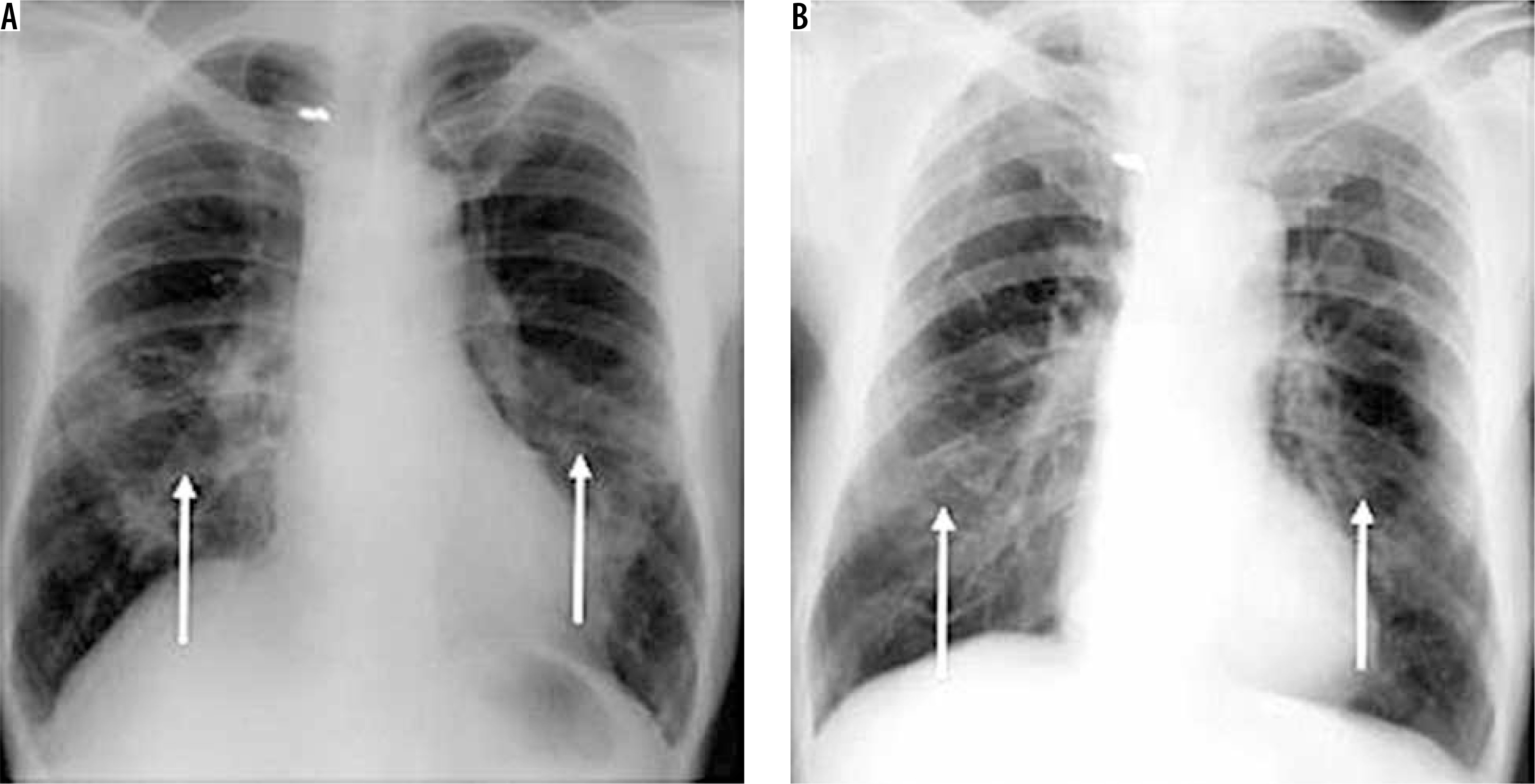
Figure 5
Chest X-ray of multidrug-resistant tuberculosis diagnosis: nodules (white arrow). Barcode number: 1221317

Table 4 shows in detail the results of the correlation analysis of lesion type, lesion location, and lesion extent on chest X-rays of NTM and MDR-TB infection. Chest X-ray lesion characteristics of NTM infection are not sufficiently specific to be a predictor of NTM occurrence because all lesions, except a mass, had a significant correlation with NTM occurrence. The lesion location that was a significant predictor of NTM infection was the left ventricular/medial field, with an OR value of 5.571, indicating that the left medial lung had a six-fold higher predictive value for NTM than the other lung sites; however, the lesion area was unrelated to NTM occurrence.
Table 4
Chest X-ray lesion characteristics of non-tuberculous mycobacteria (NTM) and multidrug-resistant tuberculosis (MDR-TB) infection
| Variable | NTM | MDR-TB | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Amount (380) | X2 square | Multivariate | Amount (11) | X2 square | Multivariate | |||||||||||||||||||
| F | % | p | OR | p | OR | F | % | p | OR | p | OR | |||||||||||||
| Lesion type | ||||||||||||||||||||||||
| Infiltrates | 39 | 7.65 | 0.000* | 0.044 | – | – | 7 | 5.0 | 0.010* | 5.053* | 0.281 | 2.147 | ||||||||||||
| Cavities | 11 | 2.16 | 0.000* | 0.065 | – | – | 4 | 7.1 | 0.021* | 5.110* | 0.232 | 2.428 | ||||||||||||
| Nodule < 3 cm | 13 | 2.55 | 0.000* | 0.118 | – | – | 5 | 11.1 | 0.001* | 9.338* | 0.003* | 18.812* | ||||||||||||
| Mass | 8 | 1.57 | 0.456 | 3.072 | – | – | 0 | 0.0 | 1.000 | – | 0.999 | 0.000 | ||||||||||||
| Consolidation | 17 | 3.33 | 0.000* | 0.066 | – | – | 4 | 5.3 | 0.057 | 3.590 | 0.194 | 0.255 | ||||||||||||
| Pleural effusion | 7 | 1.37 | 0.000* | 0.131 | – | – | 1 | 4.0 | 0.417 | 2.054 | 0.866 | 1.234 | ||||||||||||
| Pleural thickening | 7 | 1.37 | 0.000* | 0.161 | – | – | 2 | 9.5 | 0.067 | 5.825 | 0.435 | 2.224 | ||||||||||||
| Fibrosis | 40 | 7.84 | 0.000* | 0.218 | – | – | 5 | 5.7 | 0.010* | 4.357* | 0.149 | 2.871 | ||||||||||||
| Calcification | 19 | 3.73 | 0.024* | 0.451 | – | – | 1 | 3.1 | 0.501 | 1.568 | 0.589 | 0.524 | ||||||||||||
| Lesion location | ||||||||||||||||||||||||
| Right superior | 57 | 11.18 | 0.133 | 0.396 | 10 | 5.6 | 0.000* | 20.774* | ||||||||||||||||
| Right medial | 26 | 5.10 | 0.500 | 2.653 | 0 | 0.0 | 0.384 | – | ||||||||||||||||
| Right inferior | 16 | 3.14 | 0.195 | 0.949 | 1 | 2.9 | 0.533 | 1.421 | ||||||||||||||||
| Left superior | 35 | 6.86 | 0.052 | 0.279 | 9 | 8.3 | 0.000* | 19.000* | ||||||||||||||||
| Left media | 27 | 5.29 | 0.001* | 5.571* | 0 | 0.0 | 1.000 | – | ||||||||||||||||
| Left inferior | 5 | 0.98 | 0.080 | – | 0 | 0.0 | 1.000 | – | ||||||||||||||||
| Lesion extent | ||||||||||||||||||||||||
| None | 33 | 6.47 | 1 | 0.3 | 0.000* | |||||||||||||||||||
| Minimal | 51 | 10 | 1 | 1.3 | ||||||||||||||||||||
| Advanced | 7 | 1.37 | 0.645 | 0.081 | 9 | 6.2 | ||||||||||||||||||
Discussion
The National TB Survey by the National Institutes of Health Research and Development – NIHRD in 2013-2014 showed the incidence of MDR-TB to be 2.04% and that of NTM to be 70.63% (Table 1). A 1980 US laboratory survey found that approximately 60% of Mycobacterium species are non-tuberculous mycobacteria (NTM), in particular, M. avium followed by M. fortuitum and M. kansasii [12]. Some of the clinical symptoms of NTM are the presence of cough for > 2 weeks, fever, and chest pains [11]. From this national TB surveillance data, it can be seen that MDR-TB cases are minimal as compared with NTM cases (2.68%). The probability of a minimum number of MDR-TBs is due to the fact that the research was conducted among a specific target population with a minimum age of 15 years, who had lived in a cluster area for at least one month, had a history of a cough for > 14 days, and had no risk of MDR-TB.
Participants in this research were dominated by people aged above 65 years for NTM and 25-34 years for MDR-TB. This is from the Zambian studies by Ali [12], Park et al. [13], and Pascalina et al. [14] showing that the highest number of NTM cases were among the elderly (> 65 years old). Age risk factors have a significant correlation with NTM incidence because the elderly have decreased immunity and a higher occurrence of chronic lung disease (COPD) [12-15]. In the present study, NTM cases were more common in males (56.79%) than in females (43.21%); however, gender factors had no significant correlation with NTM occurrence.
Several studies have shown that most MDR-TB cases occur in people between 25 and 34 years of age, which is consistent with other studies that have shown a significant correlation between age (39.0 ± 17.3 years old) and MDR-TB incidence. In general, studies have shown that the age of NTM occurrence is higher than that of MDR-TB occurrence, and several other studies have found that there is no significant correlation between age or gender concerning either NTM or MDR-TB occurrence [16]. Several studies have found that NTM cases occur at an equal rate in both rural and urban areas [17,18]. However, in the present study, MDR-TB is more common in rural than in urban areas. The results of the present study and those from other studies indicate that residing in an urban or rural area does not affect the incidence of MDR-TB or NTM, while a low educational level appears to affect the incidence of MDR-TB and NTM.
Cough was the most common clinical symptom in NTM. This is from a Zambian study by Pascalina et al. [14], which found that the most common clinical symptoms that had a significant correlation with NTM incidence were a cough followed by chest pain, fever at night, and weight loss. In another study, the most common clinical symptoms that had a significant correlation with NTM infection were cough, phlegm cough (91-93%), and shortness of breath [13,16].
Chest X-ray lesion characteristics were highly variable, and no specific lesion could predict NTM infection. A plethora of studies have been conducted in several countries including Korea, China, the US, India, and other Asian countries showing that chest X-ray lesion characteristics of NTM are highly variable, non-specific, and highly dependent on the NTM species [6,12,19,20]. Research correlation between lesion type, lesion location, and lesion extent on chest X-ray and NTM occurrence has mostly been derived from descriptive studies that obtained the most common lesion type in NTM infection in percentage form. Analytical studies regarding the significant correlation between lesion type on chest X-ray and NTM are insufficient.
Several studies have suggested that the chest X-ray lesion with the highest prevalence in NTM infection is the reticulonodular lesion (40%) [13,21,22]. Research by Ali [12] showed that the most common lesion in NTM is the fibrocavitary lesion (90%). Other studies found that the most common lesion in NTM is the nodular lesion [12,14]. According to Piersimoni and Scarparo [20], different lesions exist in NTM infection depending on the species. The cavity and bronchiectasis lesions are most commonly found in M. avium complexes, cavities in M. kansasi, and cavities and nodules in M. celatum, M. simiae, and M. xenopi. It was previously reported that the locations of the most common lesions that have predictive power for the occurrence of NTM are the right medial lobe and the left lingula; with some studies mentioning only the medial lobes [12,13].
The studies mentioned above conclude that most chest X-ray lesions in NTM cases are fibrocavitary, bronchiectasis (BE), thin-walled, and reticulonodular cavities, with the most common location being the right medial lobe and lingula or the right and left medial lobes [10,11,15]. However, in the present study, specific/significant lesions on chest X-rays of NTM cases did not exist because infiltrates, cavities, nodules, consolidations, pleural thickening, pleural effusions, fibrosis, and calcification were all significant (p < 0.05).
Table 5 shows chest X-ray lesion characteristics of MDR-TB, and NTM incidence is explained in greater detail concerning the differences between the present and previous studies. In contrast to previous studies, the significant lesion of NTM in the present study was varied and non-specific (indistinguishable). The lesion in this study was only located in left medial lung lobe whereas there were three other types in previous studies. Thus, there were a novel information of lesion’s characteristics either NTM or MDR-TB.
Table 5
Differences in chest X-ray lesion characteristics of multidrug-resistant tuberculosis (MDR-TB) and non-tuberculous mycobacteria (NTM) between the present and previous studies
| Radiographic finding | Present research | Previous research [4,11-13,18-20] |
|---|---|---|
| MDR-TB | ||
| Significant lesions/frequent | Infiltrates Cavities Nodules Pleural thickening | Small nodules Multiple cavities with thick walls Bronchiectasis (BE) |
| Lesion location | Right superior and left superior | All over the lungs (diffuse) |
| NTM | ||
| Significant lesions/frequent | Varied, non-specific | Thin-walled cavities (MAC) Fibrocavitary lesions Bronchiectasis (BE) Reticulonodular cavities |
| Lesion location | Left medial lung lobe | Right medial lung lobe Lingula Medial lung lobes (left or right) |
Conclusions
This research concluded that chest X-ray lesion characteristics of MDR-TB show significant correlation among cavities, nodules, and fibrosis. Of these three MDR-TB lesion characteristics, the presence of a nodule is the best predictor. Location in the right superior and left superior lungs shows a significant correlation with MDR-TB incidence, while the lesion extent on chest X-ray shows no significant correlation. Chest X-ray lesion characteristics of NTM do not indicate a specific lesion because all lesions except a mass indicate a meaningful correlation. The most common lesion location in NTM incidence is the left medial lung, although statistically, the location of the lesion did not indicate a significant relationship with the incidence of NTM.