Introduction
According to some studies, cycling predisposes to the ulnar neuropathy referred to as “cyclist’s palsy” [1,2]. It is theorised that the forced prolonged extension of the wrist that results from holding the handlebars of the bicycle exposes the nerve to increased pressure in the Guyon’s canal or, more distally, in the area of nerve’s motor branch [1,2].
The forced extension of the wrist due to the position of the hands on the handlebars of a bicycle is a significant factor in exposing the nerves of the upper limb to pressure, most often at the level of Guyon’s canal or in the area of the nerve’s motor branch [1-3]. It has been reported that intensive training can lead to sensory and motor symptoms that share similarities with ulnar tunnel syndrome (UTS) in Guyon’s canal [2]. Typically, these symptoms depend on the section of the nerve that is being compressed [4,5] and disappear with rest [6]. Interestingly, the median nerve is compressed even less often despite its location in the middle of the wrist, where it traverses the carpal tunnel and where the hand rests on the handlebar. However, during long-term cycling, cyclists can experience not only ulnar nerve compression and its associated symptoms but also impairments in grip strength and sensory changes typical of median nerve disorders [7]. Conduction blockade in both nerves is probably rare, but reports of the use of electrodiagnostic examination (EDX) have been sparse [8]. Recently, shear wave elastography (SWE) has been shown to have valuable diagnostic charac-teristics in carpal tunnel syndrome (CTS) [9]. It enables quick and objective assessment of changes in the nerve, allowing for conclusions about their nature [8]. This study aimed to assess potential changes in the elasticity of the median nerve compared to the ulnar nerve in training cyclists, and to present these alterations in accordance with established elastographic standards for nerve stiffness.
Material and methods
The study was conducted at a tertiary university hospital in accordance with the 1975 Declaration of Helsinki. The study protocol (103/2018) was approved by the Local Bioethics Committee, and written informed consent was obtained from all participants.
The study included a group of cyclists and 2 reference groups that included a group of healthy volunteers and a group of ulnar nerve entrapment individuals with symptomatic cubital tunnel syndrome. Cyclists were recruited through social networks and met the inclusion criterion of cycling a minimum distance of 100 kilometres per week for at least a year. All volunteers underwent physical examination, including Phalen’s, Froment’s, and Durcan’s tests to exclude subjects with symptoms of CTS and UTS/cubital tunnel syndrome. Each cyclist completed a 2-hour bicycle training session at their own intense pace. Before and immediately after the training, a clinical examination, ultrasonography, and elastographic examinations were performed. The first reference group consisted of non-cycling fellows and residents from the hospital, who were age-matched with the cyclists. All participants underwent clinical examination to exclude the presence of cubital tunnel syndrome or CTS. The second reference group included patients with sensory disturbances in the IV and V fingers caused by ulnar nerve entrapment at the cubital or ulnar tunnel level, confirmed with EDX. Individuals with coexisting CTS were excluded.
Each participant underwent conventional ultrasonography, performed by a radiologist with more than 5 years of experience, with SWE conducted using a Toshiba iAplio 900 US equipped with a 5-18 MHz transducer (Canon Medical Systems, Japan). Both upper limbs were examined. The examination was performed in a seated position, with the subject arm relaxed and forearm resting on the knee in a supine position. To measure the cross-sectional area (CSA) of the nerve (in mm2), transverse cross-sections of the ulnar nerve were acquired at the Guyon’s canal level, and of the median nerve at the carpal tunnel level. Then, the transducer was rotated 90 degrees to obtain SWE-mode images in a longitudinal axis. Measurements were acquired with the nerve positioned in the centre of the region of interest. Median and ulnar nerve stiffness was measured at the same previously marked levels.
The normality of the distribution of the analysed variables was verified using the Shapiro-Wilk test. Statistical characteristics of the analysed variables are presented as arithmetic means, standard deviations (SD), medians, minimum and maximum values, as well as lower and upper quartile values. The Mann-Whitney U test was used to compare differences between the 2 groups. The Kruskal-Wallis test with Bonferroni post-hoc test was used to compare differences between more than 2 groups. The strength and direction of relationships between pairs of variables were assessed based on Spearman’s rank correlation coefficient (R). The significance level α = 0.05 was used for comparisons between groups and for demographic charac-teristics. All calculations were performed using the Statistica 10 package (StatSoft, USA).
Results
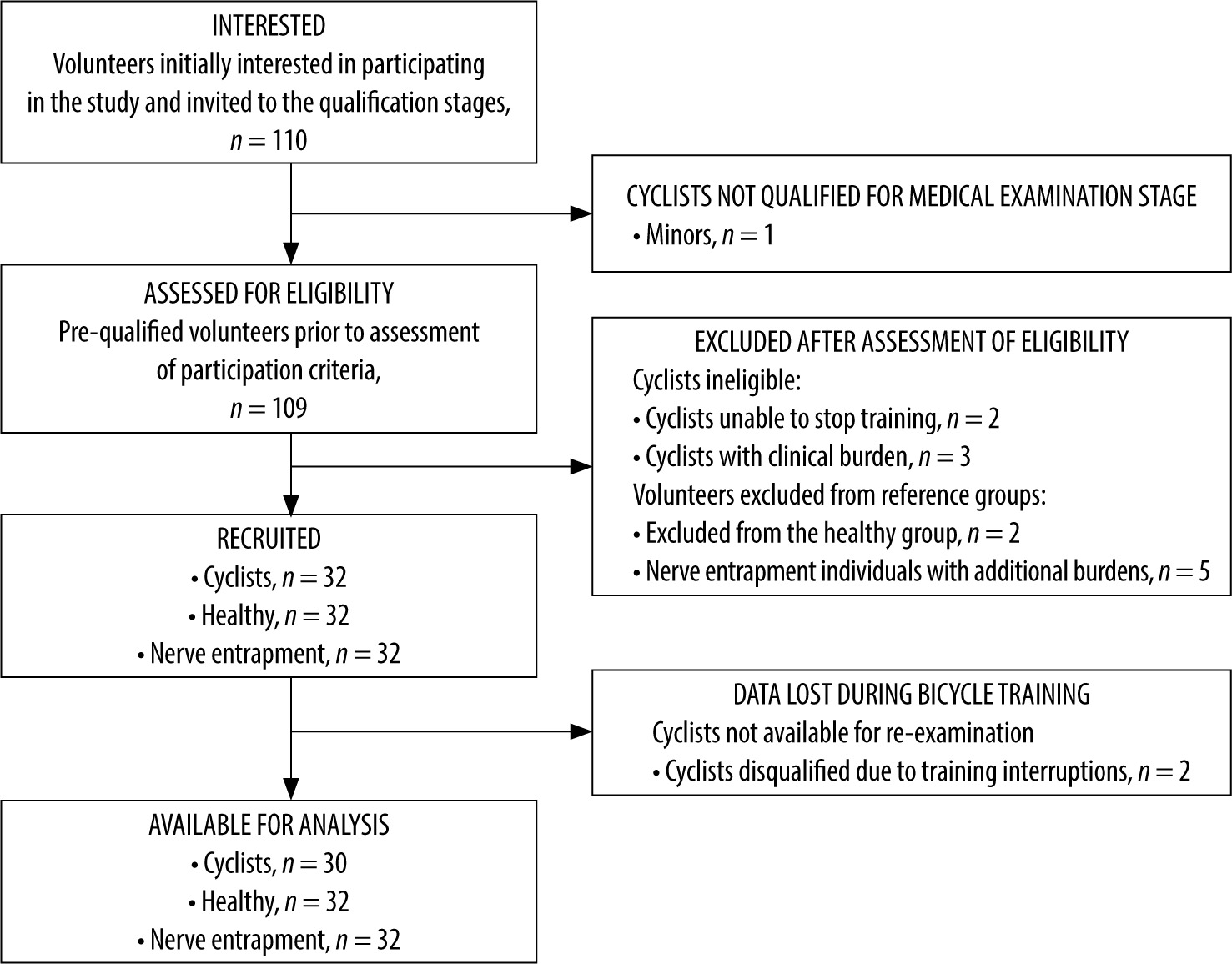
The study included 30 cyclists (26 men and 4 women, age 37.73 ± 8.92 years, BMI 24.01 ± 2.27), 32 healthy volunteers without ulnar nerve pathology (27 men and 5 women, age 36.56 ± 8.48 years, BMI 26.03 ± 1.99), and 32 ulnar nerve entrapment individuals (27 men and 5 women, age 36.03 ± 9.70 years, BMI 25.44 ± 1.79) (Table 1). The number of participants in the subsequent stages of recruitment is presented in the flow diagram (Figure 1). The only statistically significant difference between groups was a lower mean BMI in the cyclist group compared to the healthy and ulnar nerve entrapment controls (p < 0.001). No significant intergroup differences were found in age and in gender distribution. No significant correlation was found between the age or BMI of the study participants and nerve CSA and stiffness. None of the cyclists exhibited symptoms of sensory disturbances or motor deficits within the area of ulnar or median nerve innervation before or after the training session.
Table 1
Demographics of study participants
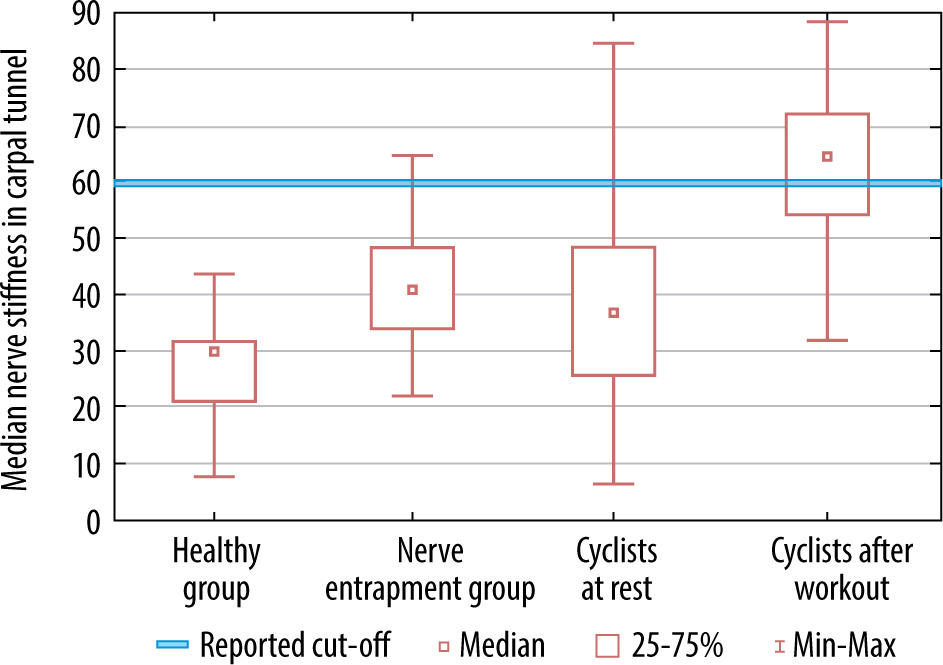
The average median nerve CSA value in resting cyclists was 9.10 mm2. This value was significantly higher than the CSA in healthy individuals (7.17 mm2, p < 0.001) and significantly higher than in the nerve entrapment group (7.86 mm2, p < 0.001) (Table 2). The average stiffness of the median nerve in cyclists before the workout was 38.54 kPa, which was significantly higher than in healthy group (27.06 kPa, p < 0.001) but not significantly different from the value in nerve entrapment group (41.50 kPa) (Table 3).
Table 2
Summary of ulnar and median nerves cross-sectional area in mm2
Table 3
Summary of ulnar and median nerves stiffness in kPa
After cycling, the average CSA value of the median nerve increased to 9.43 mm2. This value was not significantly different from the CSA value at rest (9.10 mm2). It was, however, higher than the mean value observed in the healthy group (7.17 mm2, p < 0.001) and higher than the value in the nerve entrapment group (7.86 mm2, p < 0.003) (Table 2) (Figure 4). The mean stiffness of the median nerve after training increased to 65.08 kPa. It was significantly higher than the resting value (38.54 kPa, p < 0.001) and higher that in both healthy group (27.06 kPa, p < 0.001) and the nerve entrapment group (41.50 kPa, p < 0.001) (Table 3) (Figure 5).
Figure 2
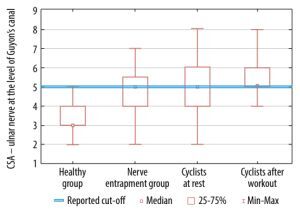
Cross-sectional area (CSA) of the ulnar nerve at the level of Guyon’s canal. Comparison of measurement parameters obtained in cyclists before and after riding, and among the healthy population and the nerve entrapment group
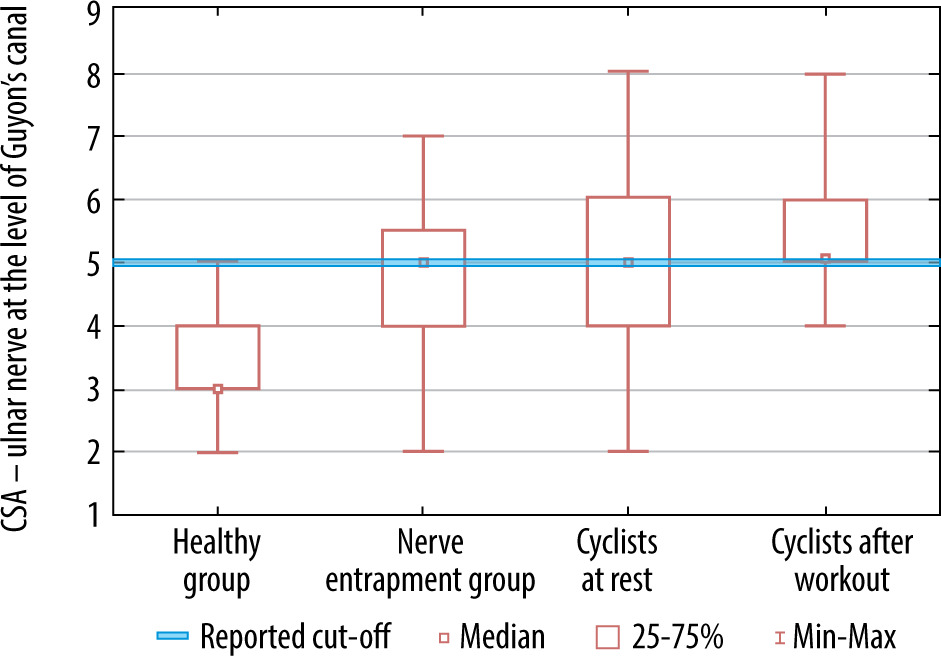
Figure 3
Stiffness of the ulnar nerve at the level of Guyon’s canal. Comparison of measurement parameters obtained in cyclists before and after riding, and among the healthy population and the nerve entrapment group
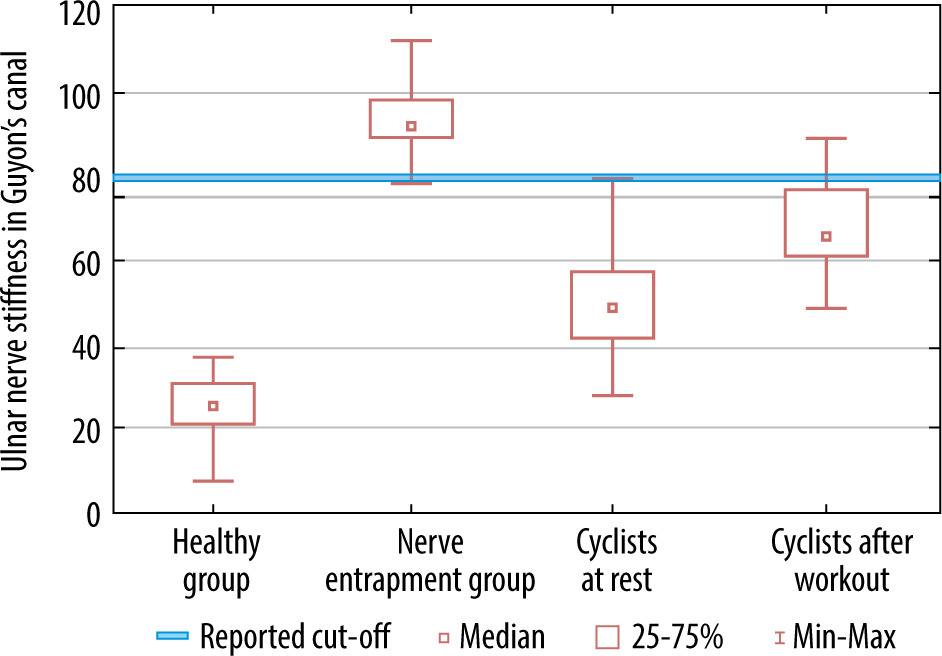
Figure 4
Cross-sectional area (CSA) of the median nerve at the carpal tunnel level. Comparison of measurement parameters obtained in cyclists before and after riding, and among the healthy population and the nerve entrapment group
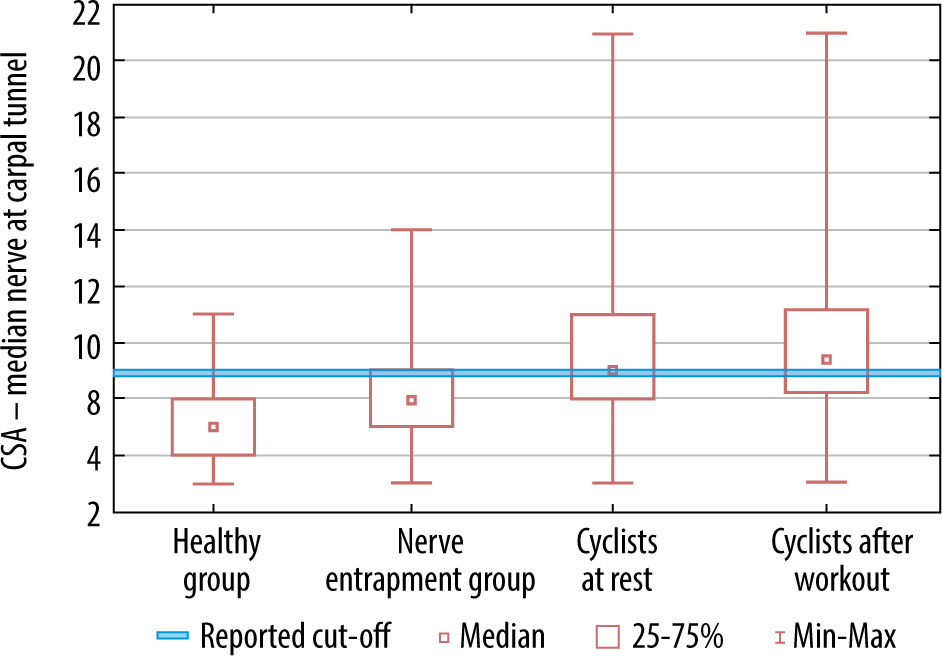
Figure 5
Stiffness of the median nerve at the carpal tunnel level. Comparison of measurement parameters obtained in cyclists before and after riding, and among the healthy population and the nerve entrapment group
The average ulnar nerve CSA value in Guyon’s canal at rest was 5.30 mm2, which was significantly higher than in healthy volunteers (3.31 mm2, p < 0.001), but did not differ significantly from the value in nerve entrapment group (4.72 mm2) (Table 2). The average stiffness of the ulnar nerve in Guyon’s canal at rest was 49.05 kPa, which was significantly higher than in healthy individuals (25.71 kPa, p < 0.001) but significantly lower than in the nerve entrapment group (94.05 kPa, p < 0.001) (Table 3).
After training, the average CSA in Guyon’s canal increased to 5.68 mm2, significantly exceeding the resting CSA value (p < 0.05) and exceeding values of both healthy and nerve entrapment groups (p < 0.001 and p = 0.004, respectively) (Table 2, Figure 2). Also, a significant increase in average stiffness was observed in comparison to the resting value (to 68.05 kPa, p < 0.001) and in comparison to the healthy group (p < 0.001) but lower than in comparison to the nerve entrapment group (p < 0.001) (Table 3, Figure 3).
Discussion
Individuals engaged in cycling sometimes experience changes in the distal sections of the ulnar nerve that cause symptoms characteristic of those suffering from compression syndromes of this nerve in Guyon’s canal [1,2]. Far less frequently, such disturbances are observed in the median nerve [6]. The pressure exerted by intensive training contributes to characteristic symptoms, which usually appear after training and disappear after a period of rest [2]. They might include sensory disturbances of the IV and V fingers or mixed sensory and motor symptoms, depending on the exact pressure site [4,5]. However, in some, even a few days of intensive cycling does not lead to clinically noticeable symptoms [8]. The lack of a reliable diagnostic method makes it impossible to evaluate morbidity in cycling sportsmen or even confidently confirm the direct correlation between this sport and CTS and UTS. The present study aimed to determine whether these sporadically observed disorders can be detected through elastographic examination. In our study we were particularly interested in the change in stiffness of the median nerve. Although this nerve appears to be exposed to pressure to a similar extent to the ulnar nerve, symptoms of median nerve disorders are less common.
Another objective of the study was to elucidate whether the observed alterations in nerve elasticity among cyclists would facilitate understanding why manifestations of median nerve compression are less prevalent than those of ulnar nerve compression.
The results observed in the median nerve of cyclists were compared to those of a group of healthy individuals, because a comparison with patients suffering from cubital tunnel syndrome seemingly lacks relevance. Pathological changes in the ulnar nerve do not directly affect the median nerve. Patients with cubital tunnel syndrome, however, have a healthy median nerve; thus, they can serve as an additional normal control group when examining the median nerve.
In the present observation the results observed in the ulnar nerve were compared to those observed in healthy individuals as well as a group of volunteers with cubital tunnel syndrome. Entrapment of the ulnar nerve in the cubital tunnel leads to chronic compression, ischaemia, and axonal conduction disorders, which can be demonstrated in electrophysiological examinations even in the distal segments of the nerve, including its passage through Guyon’s canal. It was therefore assumed that the nerve pathology at the elbow level would also be detectible at the level of the Guyon’s canal. Comparing a group of such patients with cyclists who have experienced wrist nerve disorders from cycling could be interesting, and it would illustrate the extent of impairments in cyclists, especially since the boundaries of pathology in the Guyon’s canal are known from other studies [10].
It was observed that the parameters of the CSA and the stiffness of the median nerve were higher in resting cyclists than in the healthy group. However, they did not exceed the values observed in the healthy median nerve within the cubital tunnel syndrome group. In the ulnar nerve in Guyon’s canal, the values of CSA and nerve stiffness in resting cyclists were also higher than in the healthy group, but they did not exceed the mean values observed in the nerve entrapment group.
The results of these parameters measured during rest are particularly interesting. Cyclists were asked to suspend their trainings for a week to ensure that any potential stimulation of the measured parameters following their recent trainings had subsided and the results of the first examination refer to the resting state. It may therefore be concluded that any nerve changes observed during rest have a persistent nature. In both Guyon’s canal and in the carpal tunnel, the observed resting changes exceeded the same parameters in the healthy group. In this situation, it is interesting to compare them with the results of other researchers [10].
In comparison to the healthy controls from this study, the median nerve of cyclists at rest had a significantly higher CSA and significantly greater stiffness. Recent meta-analyses reported that the pooled estimate of the CSA at carpal tunnel inlet is 8.54 mm2 [11] or 8.3 mm2 [12]. The values observed in the current study are consistent with these reports, as the normal young volunteers mean CSA was estimated at 7.17 mm2 and the values of resting cyclist at 9.10 mm2 (Table 2, Figure 4).
The norms of stiffness of the median nerve have been determined by various authors [13,14]. A summary of previous observations was also conducted in a meta-analysis [14] and in a comparison of different elastography techniques [15]. In the early observations the average stiffness of the nerve in a healthy population was observed at 32 kPa and the cut-off value proposed for 40.4 kPa [14]. Other researchers observed that the normal values are higher: 36.8 kPa [16], 43.6 kPa [17], reaching even 83.5 kPa [18]. The cut-off values were proposed at 57 kPa and 79 kPa [19,20]. The stiffness of the median nerve in resting cyclists falls therefore within the lower range of norms presented in the literature, although it is significantly higher than the value observed in the current healthy group but not higher than the values in the ulnar nerve entrapment group (Table 3, Figure 5).
There are few data on ultrasonographic norms in the area of Guyon’s canal. According to various reports, the CSA of a healthy nerve ranges from 3.92 to 4.82 mm2 and more [18,21,22]. Values now observed in the healthy (3.31 mm2) group are therefore below the lower limits of the established normal range. The values of the nerve entrapment group (4.72 mm2) are within normal limits, while the values in resting cyclists (5.30 mm2) are slightly above the cut-off value for CSA proposed for 5 mm2 [10](Figure 2).
The mean normal nerve stiffness in the Guyon’s canal value was estimated at 49.08 kPa and the cut-off value at 80 kPa [3,10]. Therefore, values observed in the present study in the healthy group may be considered as low, which may result from the differences in age of the participants in both studies. The values observed in resting cyclists (49.05 kPa) are normal (Table 3, Figure 3).
Cycling workout has an uneven effect on both studied parameters. The values of CSA observed in the median nerve within the carpal tunnel and in the ulnar nerve within the Guyon’s canal increase, although these changes are weak or insignificant (Figures 2 and 4). Our study shows that cycling increases stiffness, suggesting that the median nerve responds in a similar way to the ulnar nerve. Comparing these 2 nerves with each other, only slight differences in their average resting stiffness can be noticed, with values for the median nerve at 38.53 kPa and the ulnar nerve at 49.05 kPa. However, it is very questionable whether this difference has an impact on the more commonly reported ulnar nerve disorders in cyclists. Post-training stiffness of both nerves in the examined areas were elevated significantly, although both values remained below maximal cut-off values presented in the literature (Figures 3 and 5). The mean value after training observed in the median nerve was estimated at 65.08 kPa and in the ulnar nerve in Guyon’s canal at 68.05 kPa. Therefore, the influence of training confirms that cycling exerts compression causing oedema in both nerves as their CSA increases. However, the rise in stiffness that depends of fibrosis [23] is pronounced more than CSA that depends on oedema. This phenomenon deserves clarification. Perhaps discrete changes in CSA are more difficult to diagnose because they are more operator dependent than SWE.
Conclusions
Neither the median nor the ulnar nerve in the wrists of cyclists appear to be affected, but they remain beyond the norms established for CSA and stiffness. In our study, we did not notice significant differences in parameters of the median nerve compared to the ulnar nerve at the wrist level, which could explain the lower frequency of median nerve disorders in cyclists. More frequently reported symptoms experienced by cyclists related to the ulnar nerve may not be primarily due to pressure on the nerve from the handlebars, but rather from other factors such as elbow positioning and tension on the ulnar nerve [3]. Furthermore, as previously noted, the median nerve benefits from protection by the robust transverse carpal ligament, which reduces its susceptibility to external compression within the carpal tunnel [2]. A cycling workout exerts compression, resulting in transient oedema of both nerves. However, the dynamics of changes is more noticeable in SWE examination than in the conventional ultrasound. It may depend on SWE sensitivity [24]. Elastography shows potential as a reliable monitoring tool for transient oedema of the nerves exposed to compression in cyclists. It can probably be used for screening nerve injuries and optimising training programs to reduce the risk of nerve impairments.
The main limitation of the current study appears to be the lack of observations regarding the resolution of oedema in both nerves over time. It was only observed that one week after the cessation of training, the values of both parameters return to the upper limits of the norms established in the literature. Another limitation is the absence of an additional control group with CTS for comparison with the median nerve in cyclists. Instead, the stiffness of the median nerves in cyclists was compared to patients with cubital tunnel syndrome with electrophysiological changes observed at the level of Guyon’s canal. However, this comparison raises new questions rather than providing clear answers.